
Current Issue: July 2026
Image Gallery
Some of this month's most significant images.
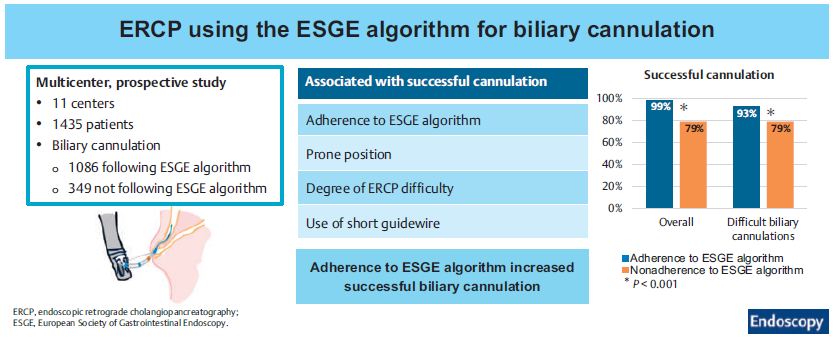
Effectiveness and safety of ERCP using the European Society of Gastrointestinal Endoscopy algorithm for biliary cannulation: a prospective study
Graphical Abstract
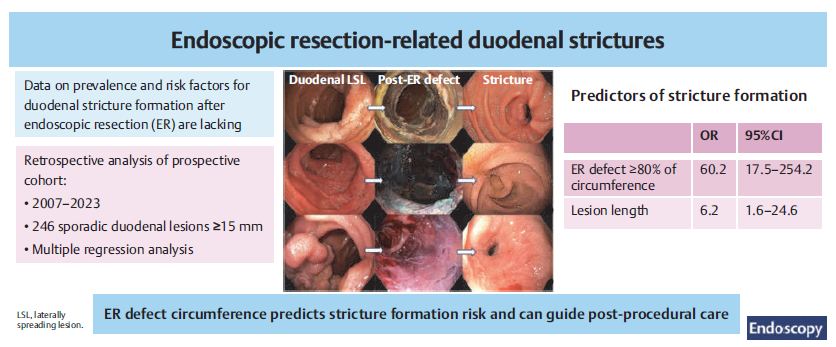
Endoscopic resection-related duodenal strictures: prevalence, risk factors, management, and outcomes
Grapical Abstract
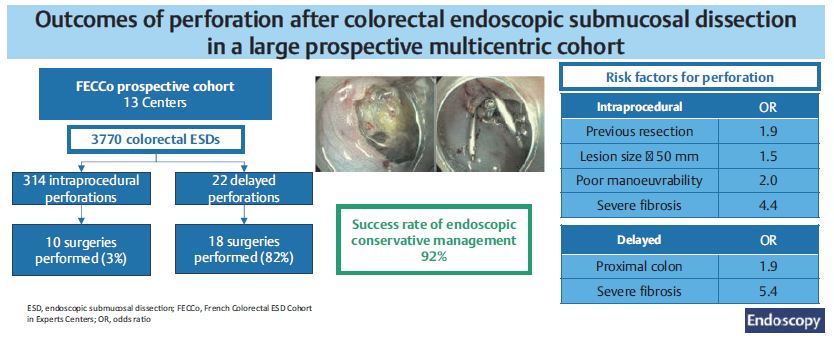
Outcomes of perforation after colorectal endoscopic submucosal dissection in a large prospective multicenter cohort
Graphical Abstract
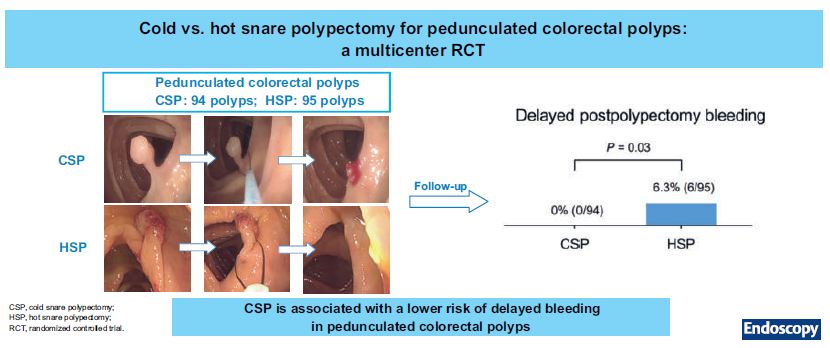
Cold versus hot snare polypectomy for pedunculated colorectal polyps: a multicenter randomized controlled trial
Graphical Abstract
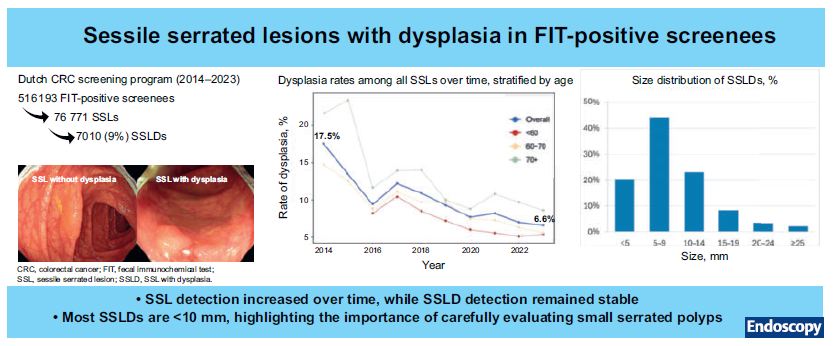
Prevalence and characteristics of sessile serrated lesions with dysplasia in Dutch fecal immunochemical test-positive screenees
Graphical Abstract
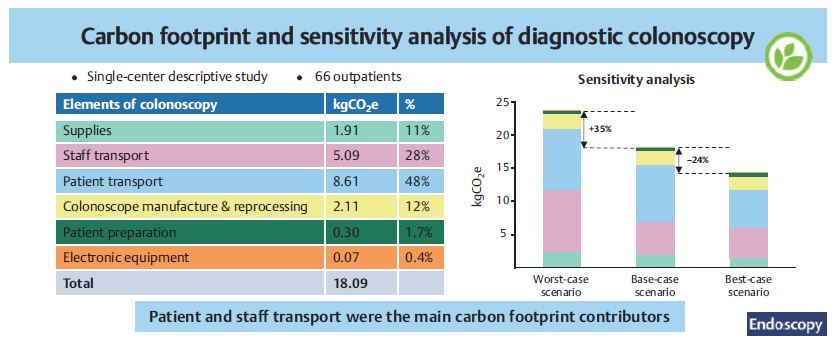
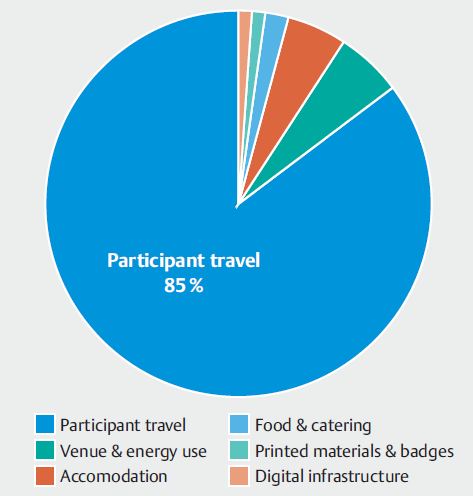
Sustainability in endoscopic medical congresses and courses: ESGE and ESGENA Position Statement
Fig. 1 Main sources of environmental impact associated with medical conferences: relative contributions.


Official organ of ESGE
Journal Impact Factor: 11.8
In this issue
Newsletter
Don't want to miss important information?
Sign up for your monthly Endoscopy-Newsletter: Our Editorial Team offers insight in what's new and important.